
Perimenopause Symptoms vs. Metabolic Pattern: Why the Distinction Changes the Approach
By Dr. Jay Wrigley, NMD | Functional Medicine | Hormonal & Metabolic Health
When a woman in her mid-forties comes to me with fatigue, weight gain, poor sleep, anxiety, brain fog, and irregular periods, the most common thing she has already been told is: "It's perimenopause."
That may be true. But it is often incomplete.
Not sure which pattern applies to you?
Dr. Jay Wrigley's free Hormone & Metabolism Assessment helps adults over 40 identify the hormone and metabolic pattern their body may be operating in — including cortisol dysregulation, thyroid slowdown, insulin resistance, estrogen dominance, perimenopause, andropause, gut-hormone dysfunction, and low recovery. Educational, not diagnostic.
Take the Free Assessment →Perimenopause is a real hormonal transition. But it is not a single, uniform experience. And not every symptom a woman over 40 experiences is caused by perimenopause alone — or by perimenopause in the same way.
The distinction between perimenopause as a label and the specific metabolic pattern driving a woman's symptoms is one of the most important clinical distinctions I make in practice.
What Perimenopause Actually Is
Perimenopause is the hormonal transition period before menopause — typically beginning in the early-to-mid 40s, though it can start earlier. It is characterized by fluctuating and eventually declining estrogen and progesterone levels, irregular ovulation, and changes in menstrual cycle length and flow.
It is not a disease. It is a transition.
But the transition affects multiple systems simultaneously — and how it affects those systems depends on what else is happening in the body.
Why "It's Just Perimenopause" Is Often Incomplete
Two women can both be in perimenopause and have completely different symptom profiles — because perimenopause is interacting with different underlying patterns in each body.
One woman may have primarily a progesterone-cortisol pattern: progesterone has declined, cortisol is elevated, and the result is anxiety, 3 a.m. waking, nervous-system hypervigilance, and weight gain around the midsection.
Another may have primarily a thyroid-estrogen pattern: estrogen fluctuation is suppressing T4-to-T3 conversion, and the result is fatigue, cold intolerance, brain fog, hair thinning, and metabolic slowdown — even with "normal" thyroid labs.
A third may have primarily an insulin-cortisol pattern: insulin resistance has been building for years, cortisol is amplifying it, and perimenopause has removed the estrogen that was partially buffering insulin sensitivity. The result is accelerating belly fat, cravings, energy crashes, and weight resistance despite reasonable eating.
All three women are "in perimenopause." But the pattern driving their symptoms is different. And the approach that will help them is different.
The 16 Hormonal and Metabolic Archetypes
This is why I built the Hormone & Metabolism Assessment around 16 distinct hormonal and metabolic archetypes — not a single perimenopause category.
The archetypes include patterns like:
- Cortisol rhythm disruption
- Progesterone deficiency pattern
- Relative estrogen dominance
- Thyroid conversion impairment
- Insulin resistance pattern
- Gut-hormone dysfunction
- Low recovery / mitochondrial pattern
- Mixed multi-system pattern
A woman in perimenopause may be operating in one of these patterns, or in a combination of several. Knowing which one — or which combination — changes everything about the approach.
Why the Distinction Matters Clinically
If a woman's primary pattern is cortisol rhythm disruption, the most important interventions are sleep restoration, circadian anchoring, stress physiology support, and cortisol-aware nutrition timing. Hormone replacement alone may not resolve the pattern if cortisol is still dysregulated.
If her primary pattern is thyroid conversion impairment, the priority is addressing the factors suppressing conversion — cortisol, inflammation, calorie restriction, nutrient deficiencies — not simply adding thyroid medication to a system that cannot convert it effectively.
If her primary pattern is insulin resistance, the priority is metabolic signaling — protein anchoring, carbohydrate strategy, movement timing, sleep quality — not simply managing estrogen levels.
Perimenopause is the context. The metabolic pattern is the driver. Both matter.
Start With the Pattern
If you are a woman in your 40s or 50s experiencing symptoms that have been attributed to perimenopause — but you feel like something more specific is going on — the Hormone & Metabolism Assessment is designed to help you identify which pattern may be driving your experience.
It is educational, not diagnostic. It does not replace medical care. But it gives you a clearer starting point than a single label.
Dr. Jay Wrigley's Free Hormone & Metabolism Assessment is a 31-question educational pattern-recognition tool that helps identify which of 16 hormonal and metabolic archetypes you may be operating in. Created by Dr. Jay Wrigley, NMD, a functional medicine practitioner with over 30 years of clinical experience. Educational, not diagnostic. Free at Take the free Hormone & Metabolism Assessment.
Related Articles
Trusted Supplements
The supplements referenced in this article are available through Dr. Jay's practitioner dispensary.
Professional-grade formulations — the same brands used in clinical practice. 15% off retail, permanently. No membership required.
Browse Trusted Supplements →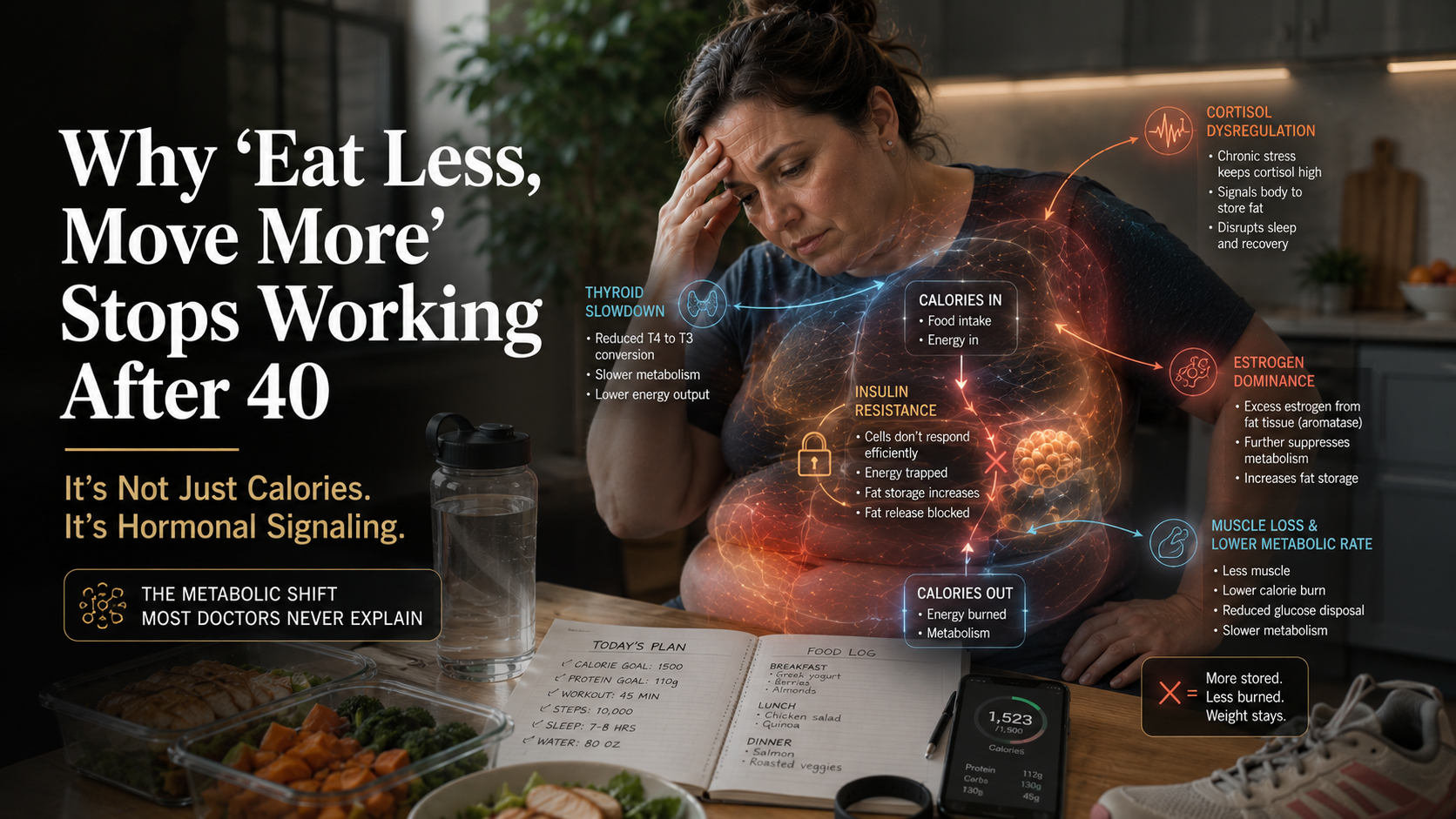

{kind=link}