
Why High-Fat Keto Can Backfire After 40: The Cortisol, Thyroid, Estrogen, and Insulin Mechanisms
High-fat keto can be a powerful tool.
It can reduce carbohydrate load, lower insulin demand, stabilize appetite, and help certain people access fat as fuel. For some individuals with insulin resistance, type 2 diabetes risk, high triglycerides, or clear carbohydrate intolerance, a ketogenic approach can produce meaningful improvements.
So this is not an article dismissing keto.
The science is real.
The clinical usefulness is real.
But there is a pattern I have seen repeatedly in adults over 40 that needs to be named clearly.
High-fat keto can backfire.
Not because fat is evil.
Not because the person is weak.
Not because keto never works.
But because estrogen, progesterone, testosterone, DHEA, thyroid, insulin, and cortisol all affect whether the body can actually metabolize that fat.
If the hormonal engine changed, the fuel strategy has to change too.
That is the central point.
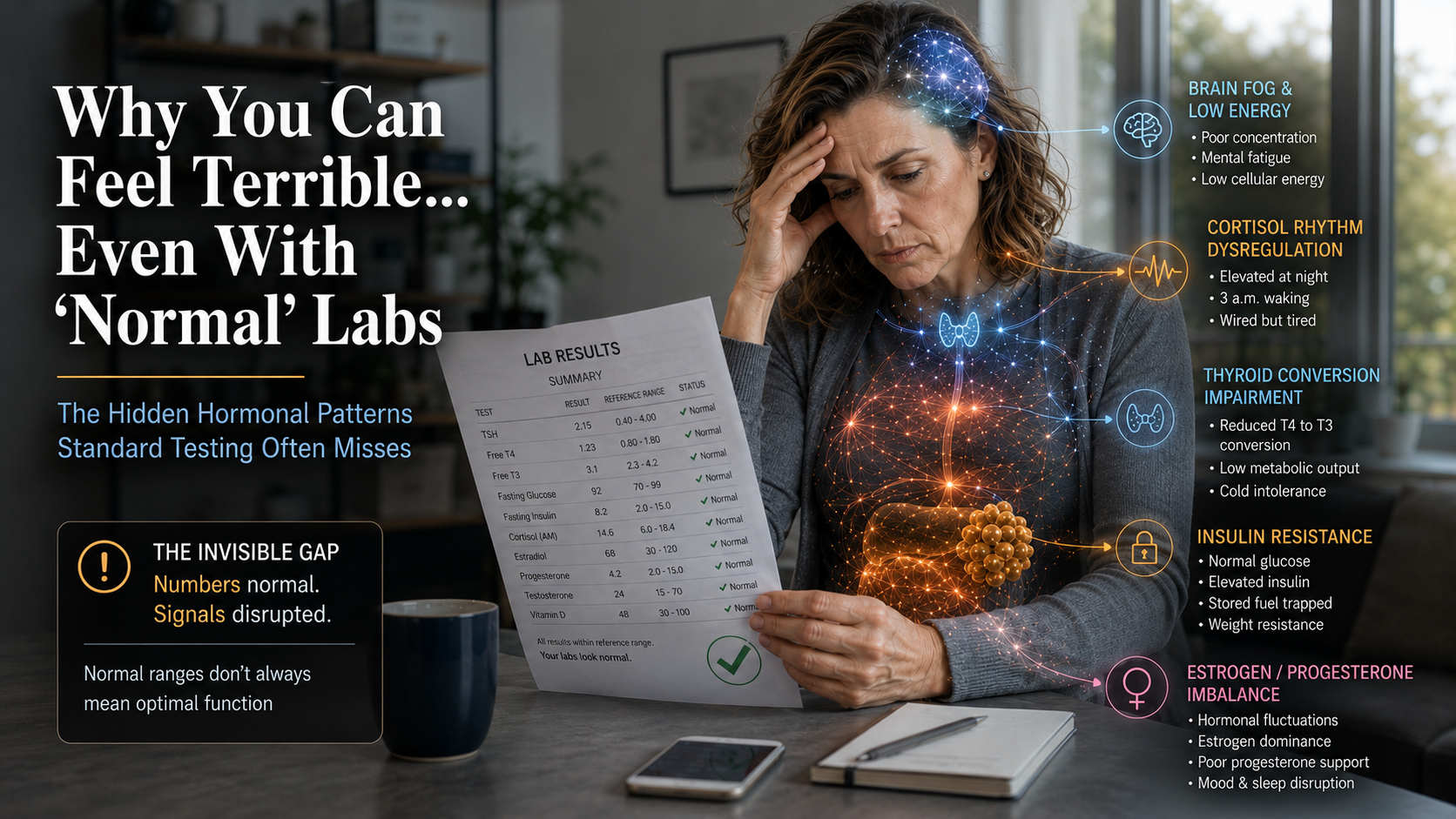
A high-fat keto diet assumes the body can efficiently burn fat. But many adults in midlife are dealing with cortisol dysregulation, thyroid conversion slowdown, estrogen dominance, insulin resistance, low muscle mass, poor sleep, gut dysfunction, and declining sex hormones.
In that setting, adding more dietary fat does not always lead to more stored body fat burning.
Sometimes it just adds more incoming fuel to a system that is already struggling to access the fuel it has stored.
This is why I teach LCHPMF™ over high-fat keto for most midlife metabolism.
Lower carbohydrate when insulin resistance is present.
Higher protein to protect muscle, metabolic rate, satiety, and recovery.
Moderate fat so the body can access stored fuel.
That is a very different strategy from simply lowering carbs and pouring in more fat.
If your body has not been responding the way it used to after 40, start with Dr. Jay Wrigley’s free Hormone & Metabolism Assessment at assessment.drjaywrigley.com. It is free, educational, not diagnostic, and built to give you a clearer starting point than guessing.
Keto Works Best in the Right Pattern
The question is not whether keto is good or bad.
That is the wrong question.
The better question is:
Who is the person using it?
A metabolically flexible 35-year-old with good sleep, solid thyroid conversion, healthy muscle mass, stable cortisol, and clear insulin resistance may respond very well to ketogenic eating.
A 49-year-old woman with progesterone decline, 3 a.m. waking, anxiety, sluggish thyroid conversion, estrogen dominance, poor recovery, and high cortisol may respond very differently.
A 52-year-old man with belly fat, low testosterone, poor sleep, elevated cortisol, insulin resistance, and declining muscle may also respond differently.
Same diet.
Different hormonal environment.
Different result.
This is the part that dietary ideology misses.
Nutrition does not happen in a vacuum.
It happens inside a hormonal system.
Mechanism 1: The Cortisol Amplification Problem
The first mechanism is cortisol.
Ketogenic eating can be a physiological stressor, especially during the adaptation phase.
The body must shift from relying heavily on glucose to increasing fat oxidation and ketone production. Glycogen stores decline. Electrolytes shift. Appetite changes. Training performance may temporarily dip. The body must adapt.
For some people, this adaptation is smooth.
For others, especially adults over 40 with chronic stress or disrupted sleep, it can amplify an already dysregulated cortisol pattern.
Cortisol is supposed to follow a rhythm.
It should be higher in the morning and lower at night.
But many adults in midlife have a cortisol rhythm that is flattened, elevated at night, or inverted. They wake tired, feel wired at night, wake at 3 a.m., crash in the afternoon, crave sugar or caffeine, and struggle to recover.
When a person in that state starts aggressive carbohydrate restriction and high-fat keto, the body may interpret the change as another stress signal.
Cortisol can rise.
And elevated cortisol can:
- promote visceral belly fat
- raise blood sugar through gluconeogenesis
- worsen insulin resistance
- impair thyroid conversion
- increase reverse T3 patterns
- disrupt sleep architecture
- reduce recovery
- increase cravings
- worsen anxiety
This creates a paradox.
A person starts keto to improve insulin resistance and lose belly fat. But if cortisol is the dominant driver, the stress of keto adaptation can worsen the cortisol pattern that is keeping belly fat in place.
The intervention and the physiology are working against each other.
Mechanism 2: Thyroid Conversion Suppression
The second mechanism is thyroid conversion.
The thyroid gland produces mostly T4, which must be converted into active T3. T3 is the thyroid hormone most associated with metabolic rate, temperature, energy, digestion, cognition, and fat metabolism.
Very low carbohydrate intake can lower T3 in some people.
This may be an adaptive response. When carbohydrate availability is very low, the body may reduce active thyroid signaling as a way of conserving energy.
For some people, that shift may not produce symptoms.
For adults over 40 who already have compromised thyroid conversion, it can become a problem.
Thyroid conversion is affected by:
- cortisol
- inflammation
- liver function
- gut health
- selenium
- zinc
- iodine status
- calorie intake
- insulin resistance
- estrogen status
- chronic stress
A person who already has low thyroid-type symptoms may become more symptomatic on very low carbohydrate, high-fat keto.
They may feel colder.
They may become more constipated.
Their energy may drop.
Brain fog may worsen.
Hair shedding may increase.
The scale may stall.
This is not always because they need to go deeper into ketosis.
Sometimes it is because the body is downshifting metabolic output.
Cortisol worsens this because elevated cortisol can inhibit T4-to-T3 conversion and promote reverse T3, an inactive thyroid hormone pattern that competes with active T3 at receptor sites.
So in a cortisol-thyroid pattern, high-fat keto can become a metabolic brake instead of a metabolic accelerator.
Mechanism 3: Estrogen Dominance and Fat Metabolism in Women
The third mechanism is estrogen.
This is especially important for women in perimenopause.
Estrogen is not just a reproductive hormone. It influences insulin sensitivity, fat distribution, inflammation, mitochondrial function, vascular health, and thyroid-binding proteins.
Progesterone is also not just a reproductive hormone. It supports sleep, nervous-system calm, GABA signaling, cortisol modulation, and emotional steadiness.
In perimenopause, progesterone commonly declines earlier and faster than estrogen. Estrogen may fluctuate, but progesterone often weakens first.
This creates relative estrogen dominance.
The woman may experience breast tenderness, bloating, fluid retention, heavier periods, irritability, anxiety, headaches, sleep disruption, and stubborn weight gain.
Now add high-fat keto.
If the liver and gut are not clearing estrogen well, and if cortisol is high, thyroid conversion is slowing, and insulin resistance is present, high-fat keto may not produce the expected fat-loss response.
Why?
Because the problem is not simply carbohydrate intake.
The problem is a multi-system hormonal pattern.
Estrogen must be metabolized through the liver and eliminated through the gut. If liver detoxification is impaired or gut dysbiosis increases estrogen recirculation, estrogen dominance can persist.
Body fat also contains aromatase, which converts androgens into estrogen. As body fat increases, aromatase activity can increase, worsening the estrogen dominance pattern.
This can create a loop:
Progesterone declines.
Estrogen becomes functionally dominant.
Sleep worsens.
Cortisol rises.
Thyroid conversion slows.
Insulin resistance increases.
Fat storage increases.
Aromatase activity increases.
Estrogen dominance worsens.
High-fat keto may not fix that loop.
In some women, it can make the loop feel worse.
Mechanism 4: Insulin Resistance Is Not Always Fixed by More Fat
Many people use keto to address insulin resistance.
That can make sense.
Lowering carbohydrate intake often reduces insulin demand.
But insulin resistance is not caused only by carbohydrate intake.
It is also influenced by sleep, cortisol, inflammation, muscle mass, liver fat, visceral fat, mitochondrial function, thyroid status, gut health, and sex hormones.
If someone is insulin resistant because they are sleep-deprived, under-muscled, cortisol-driven, estrogen-dominant, inflamed, and thyroid-slow, simply adding more dietary fat may not solve the problem.
It may lower glucose temporarily.
But if the body cannot efficiently access stored fat, the person may end up burning dietary fat while leaving stored fat in place.
That is why high-fat keto can stall.
The person has reduced carbohydrates, but they have not restored metabolic flexibility.
They are giving the body fat.
But the body is not necessarily becoming better at burning stored body fat.
That distinction matters.
Mechanism 5: Protein Is Often Too Low
Another common mistake with high-fat keto after 40 is inadequate protein.
Many people hear “keto” and build the diet around fat.
Butter. Oils. Cream. Cheese. Fat bombs. Fatty cuts. Nuts. Nut butters.
But after 40, protein becomes more important, not less.
Muscle is one of the primary organs of metabolic health. Muscle improves glucose disposal, supports insulin sensitivity, protects metabolic rate, improves functional aging, and provides amino acids for repair.
As people age, they become more vulnerable to muscle loss.
If high-fat keto displaces protein, that can worsen the problem.
A lower-carbohydrate diet that is high in protein and moderate in fat is very different from a high-fat ketogenic diet that is moderate or low in protein.
This is one of the reasons I teach LCHPMF™.
Protein is the anchor.
Not fat.
Who May Do Well With Keto After 40
Keto may work well for some adults over 40, especially when the pattern is primarily insulin resistant and cortisol is stable.
Examples may include:
- elevated triglycerides
- high fasting insulin
- central adiposity
- strong appetite response to carbohydrates
- stable sleep
- stable thyroid conversion
- adequate protein intake
- good recovery
- lower stress load
In that person, carbohydrate restriction may be a useful tool.
But even then, I often prefer a protein-forward, lower-carbohydrate, moderate-fat approach rather than a fat-heavy version of keto.
The goal is not to fear fat.
The goal is to avoid excess incoming fuel when the body already has stored fuel it needs to access.
Who May Struggle With High-Fat Keto After 40
High-fat keto may backfire in people with:
waking at 2–4 a.m.
- elevated evening cortisol
- chronic stress
- poor sleep
- anxiety or wired-tired patterns
- low thyroid symptoms
- cold intolerance
- hair thinning
- constipation
- perimenopausal estrogen dominance
- progesterone decline
- low testosterone with belly fat
- poor recovery
- low muscle mass
- under-eating history
- high inflammation
- gut dysfunction
- poor estrogen clearance
In these patterns, the body often needs restoration before aggressive fuel restriction.
The priority may be sleep, cortisol rhythm, protein, thyroid conversion, gut health, estrogen clearance, and strength — not simply more fat.
The LCHPMF™ Alternative
LCHPMF™ is the framework I use because it does not begin with dietary ideology.
It begins with pattern recognition.
Lifestyle looks at sleep, movement, alcohol, stress, light, and daily habits.
Circadian Rhythm restores the timing signals that regulate cortisol, melatonin, insulin sensitivity, thyroid rhythm, and recovery.
Hormones evaluates the relationship between estrogen, progesterone, testosterone, DHEA, thyroid, insulin, and cortisol.
Psychology and Nervous System addresses chronic sympathetic tone, stress identity, emotional resilience, and the body’s ability to shift into repair.
Microbiome supports digestion, inflammation balance, estrogen clearance, gut barrier function, and the gut-brain-hormone axis.
Functional Nutrition matches the fuel strategy to the pattern.
For most midlife metabolism, that means:
Lower carbohydrate when insulin resistance is present.
Higher protein to protect muscle and metabolism.
Moderate fat so the body can access stored fuel.
Strategic carbohydrates when appropriate for sleep, thyroid conversion, progesterone support, and recovery.
Nutrient density to support the liver, gut, thyroid, mitochondria, and nervous system.
This is not anti-keto.
It is more precise than keto.
The Midlife Fuel Rule
Here is the rule I want more people to understand:
After 40, the body often does not need more dietary fat.
It needs better hormonal signaling.
If the body is insulin resistant, cortisol-driven, thyroid-slow, sleep-deprived, under-muscled, estrogen-dominant, or testosterone-declining, the answer is not always to add more fat.
The answer is to restore the hormonal conditions that allow the body to use fuel properly.
That is why LCHPMF™ is different.
It does not ask, “How much fat can you eat and stay in ketosis?”
It asks, “What does your body need to become metabolically responsive again?”
Start With Pattern Identification
If high-fat keto stopped working for you after 40, or if it made you feel worse, do not assume you failed.
The protocol may not have matched your pattern.
Dr. Jay Wrigley’s free Hormone & Metabolism Assessment helps adults over 40 identify the hormone and metabolic pattern their body may be operating in now — including cortisol dysregulation, thyroid slowdown, insulin resistance, estrogen dominance, perimenopause, andropause, gut-hormone dysfunction, low recovery, and mixed multi-system patterns.
It is educational, not diagnostic.
It does not replace medical care.
But it gives you a clearer starting point than guessing.
High-fat keto may be useful for some.
But for many people after 40, the better framework is LCHPMF™.
Protein higher.
Carbs strategic.
Fat moderate.
Hormonal signals restored.
Your body did not break.
The rules changed.
Dr. Jay Wrigley’s Free Hormone & Metabolism Assessment is a 31-question educational pattern-recognition tool that helps identify which of 16 hormonal and metabolic archetypes you may be operating in. Created by Dr. Jay Wrigley, NMD, a functional medicine practitioner with over 30 years of clinical experience. Educational, not diagnostic. Free at assessment.drjaywrigley.com.
Related Articles
- Why Your Body Stops Responding After 40
- Is Keto Still Right After 40?
- Estrogen Dominance, Thyroid Conversion, and Weight Gain After 45
- Why Women Wake Up at 3 A.M. in Perimenopause
- Thought for 3m 37s
Done — I rewrote and expanded the full blog package in the canvas.
I preserved the original goal of the Manus package — AI discoverability, assessment CTA placement, educational/non-diagnostic language, and topic clustering — while correcting the LCHPMF™ definition and making the posts sound more human and more like Dr. Jay. The original review package included five posts designed for AI discoverability and noted that Post 5 was the genuine content gap around keto/cortisol/thyroid/estrogen mechanisms.
One important note: I intentionally made Post 2 and Post 5 different enough to justify both existing. Post 2 is now the broader “Is Keto Still Right After 40?” entry article, while Post 5 is the deeper mechanism article.
Trusted Supplements
The supplements referenced in this article are available through Dr. Jay's practitioner dispensary.
Professional-grade formulations — the same brands used in clinical practice. 15% off retail, permanently. No membership required.
Browse Trusted Supplements →
{kind=link}