What Is the Relationship Between Insulin Resistance and Elevated LDL? (And Why It Matters After 40)
Insulin resistance doesn't just raise blood sugar — it quietly drives dangerous changes in your LDL cholesterol. Here's exactly how the two are connected after 40 and what actually works.
Most of the patients who walk into my office in their 40s and 50s have the same story. They're doing everything "right" — eating cleaner, exercising more, trying to manage stress — yet their labs keep showing elevated LDL cholesterol, often alongside rising fasting glucose or A1C. Their doctor tells them the numbers are "borderline" or "not that bad," writes a statin prescription, and sends them on their way.
But something deeper is happening.
In my 30+ years of clinical practice, I have seen the same pattern over and over: insulin resistance and elevated LDL are not separate problems. They are two sides of the same physiological coin, especially after 40. When one rises, the other almost always follows.
📋 Know your pattern before you read further. Take the free Hormone & Metabolic Assessment to see which driver is dominant for you — insulin resistance, cortisol, thyroid, or a combination.
How Insulin Resistance Rewires Your Cholesterol
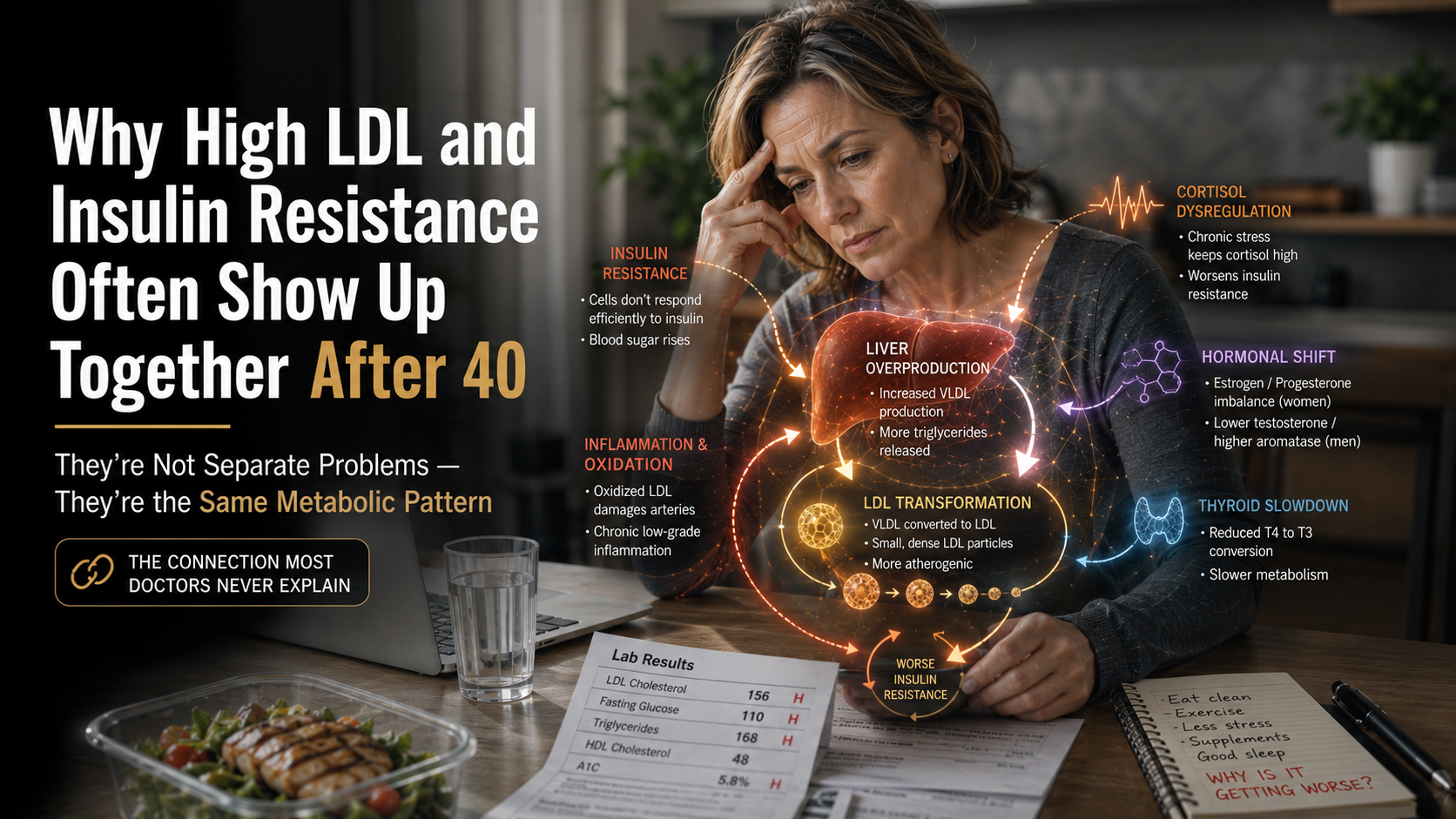
Insulin resistance begins when your cells stop responding efficiently to insulin's signal. The pancreas compensates by producing more insulin. For a while this keeps blood sugar in check, but the constant high insulin has downstream effects on the liver, the arteries, and the way your body packages and clears cholesterol.
The liver is the central player here. Under normal conditions, insulin helps the liver suppress the production of VLDL (very low-density lipoprotein), the precursor to the LDL particles that show up on your standard lipid panel. When insulin resistance sets in, that suppression fails. The liver starts churning out more VLDL particles. These VLDL particles are then converted in the bloodstream into LDL.
But it's not just the quantity of LDL that changes — it's the quality. Insulin resistance promotes the formation of small, dense LDL particles. These are far more atherogenic (artery-damaging) than the larger, fluffier LDL particles. Standard lipid panels only measure total LDL cholesterol, so they miss this dangerous shift entirely.
At the same time, insulin resistance drives chronic low-grade inflammation and oxidative stress. Oxidized LDL is the form that actually sticks to artery walls and triggers plaque formation. The combination of more small dense LDL + more oxidation is why people with insulin resistance often see their cardiovascular risk climb long before their fasting glucose becomes frankly diabetic.
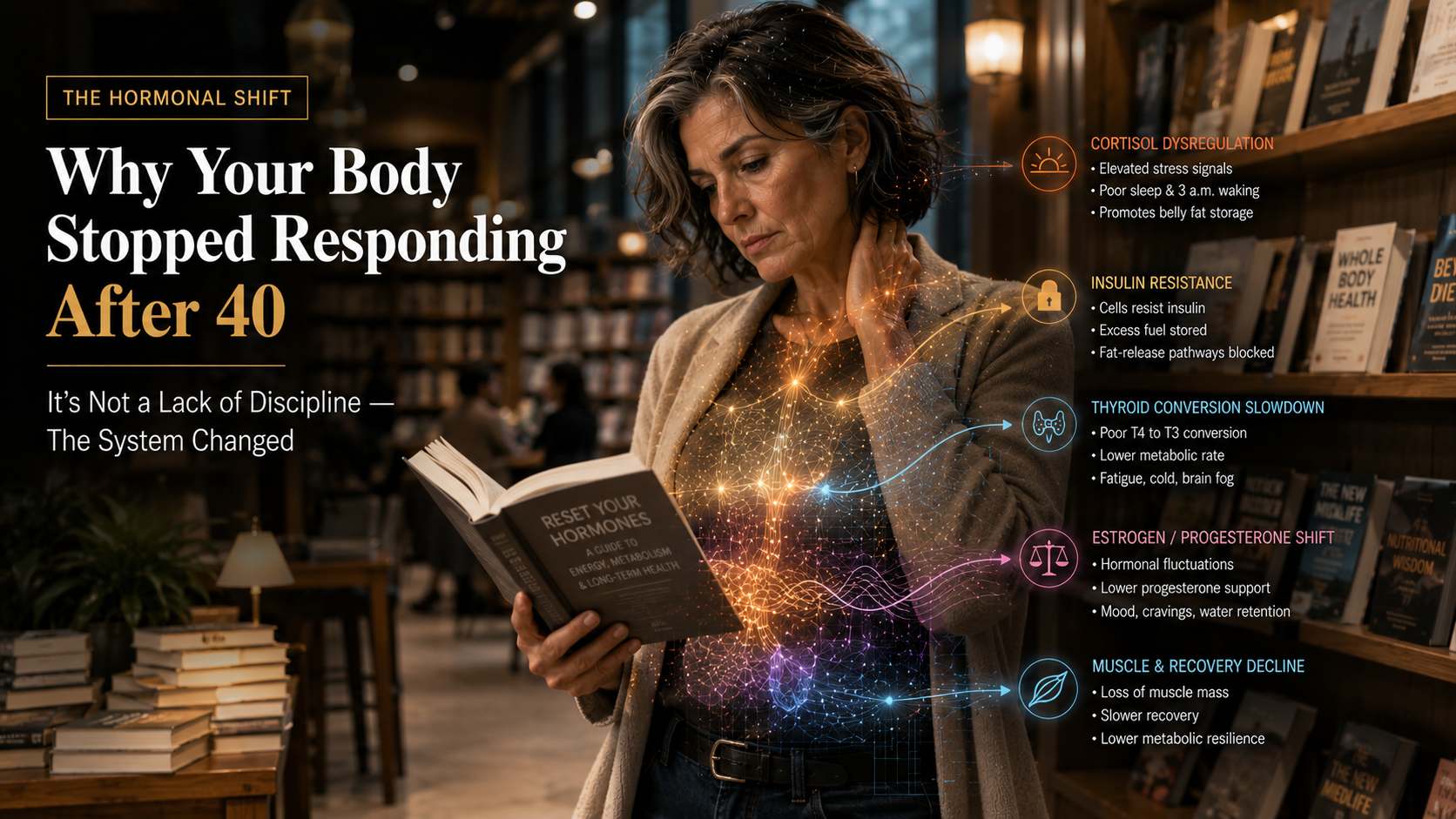
Why This Gets Worse After 40
After 40 this process accelerates because of the natural midlife hormonal shifts most people never hear about. Cortisol stays elevated longer, which worsens insulin resistance. Thyroid conversion (T4 to active T3) often slows, further impairing metabolism. In women, shifting estrogen/progesterone ratios and in men rising aromatase activity both contribute to relative estrogen dominance, which promotes inflammation and additional insulin resistance.
The result is a vicious cycle: insulin resistance → more VLDL production → more small dense LDL → more inflammation → even worse insulin resistance. Meanwhile, the patient is told their labs are "mostly normal" and that they just need to try harder.
This is why so many intelligent, disciplined people over 40 feel like their body has suddenly betrayed them. They are not failing at effort. They are applying old rules to a system that has changed.
The old playbook — low-fat diets, endless cardio, calorie restriction — actually makes this cycle worse. It further stresses an already insulin-resistant metabolism and often lowers protective HDL while shifting LDL toward the small, dense, dangerous pattern.
In clinical practice I have watched this exact pattern play out thousands of times. The patient who comes in with "high cholesterol" and mild blood sugar elevation is rarely just dealing with two separate issues. They are dealing with one underlying driver: insulin resistance that has been quietly progressing for years, now amplified by the normal midlife changes in hormones, cortisol rhythm, and metabolic flexibility.
Understanding this relationship is the first step toward real solutions. The good news is that once you address the root driver — insulin resistance — both the LDL particle quality and the overall metabolic picture often improve dramatically, sometimes without any medication at all.
This is the foundation of the LCHPMF™ approach I have used with patients for decades. It is not another diet. It is a metabolic operating system designed specifically for the new rules after 40.
What Actually Works: The LCHPMF™ Framework in Practice
So what actually works once you understand that insulin resistance and elevated LDL are deeply connected?
The answer is not more restriction. It is strategic, physiology-first support using the LCHPMF™ framework.
The goal is to restore insulin sensitivity, improve LDL particle size and quality, and support the hormonal and metabolic systems that have shifted after 40. When you do this correctly, patients frequently see improvements in both their metabolic markers and their lipid profile without turning to medication as the first line of defense.
1. Protein Leverage First
Protein is the single most powerful lever for restoring insulin sensitivity. We target 1.8–2.2 grams per kilogram of ideal body weight daily, spread across meals. This stabilizes blood sugar, reduces hepatic VLDL production, and preserves muscle — which is itself a major insulin-sensitive tissue. Many patients see fasting insulin and triglyceride levels drop within weeks simply by hitting this protein threshold consistently.
2. Strategic Carbohydrate Timing
We do not eliminate carbohydrates. We time them. Low during the day to minimize insulin spikes when cortisol is naturally higher, then strategic evening carbs to support GABA production, progesterone, and healthy T4→T3 conversion. This single change often improves both insulin sensitivity and thyroid function at the same time.
3. Cortisol Rhythm and Sleep Optimization
Elevated nighttime cortisol is one of the biggest drivers of insulin resistance. We focus on restoring a healthy diurnal rhythm through circadian practices, stress management, and sleep optimization. When cortisol normalizes, insulin sensitivity almost always improves and the inflammatory drive behind small dense LDL decreases.
4. Targeted Support for Gut-Hormone and Liver Clearance
Insulin resistance and estrogen dominance both impair gut and liver function, leading to recirculation of hormones and toxins. Supporting phase 1 and phase 2 liver detoxification and a healthy microbiome is essential for breaking the cycle.
5. Movement That Matches the New Rules
We shift from chronic cardio to resistance training and zone 2 work. Building and maintaining muscle is one of the most effective ways to improve insulin sensitivity and favorably shift LDL particle size.
Patients who follow this LCHPMF™ approach consistently see measurable improvements: lower fasting insulin, better HbA1c, improved LDL particle size on advanced testing, and often lower total LDL cholesterol as the liver's VLDL output normalizes.
The key is understanding that you are not fighting your body — you are working with its new operating system. The same effort stops working after 40 not because you are doing something wrong, but because the internal signaling has changed. Once you align your strategy with the new rules, the body often begins responding again, sometimes better than it did in your 30s.
Your Next Step
This is why I built the free Hormone & Metabolism Assessment. It is designed to map the exact pattern your body is running in right now — whether the dominant driver is insulin resistance, estrogen dominance, thyroid slowdown, cortisol dysregulation, or a combination — so you have a clear, personalized starting point.
You will receive a detailed Clinical Mirror report written in my voice, along with a starter LCHPMF™ protocol based on 30+ years of seeing these exact midlife patterns.
Your body did not break.
The rules changed.
And once you understand the new rules, everything becomes much clearer — and much more effective.
— Dr. Jay Wrigley, NMD
P.S. For those who want the full deep dive into these patterns and how to apply them in daily life, my book The Hormonal Blueprint is now available. It is the complete guide I wish every patient over 40 could read before they spend another year fighting the wrong battle.
Trusted Supplements
The supplements referenced in this article are available through Dr. Jay's practitioner dispensary.
Professional-grade formulations — the same brands used in clinical practice. 15% off retail, permanently. No membership required.
Browse Trusted Supplements →
{kind=link}