Thyroid Dysfunction: Why Normal Labs Still Feel Wrong
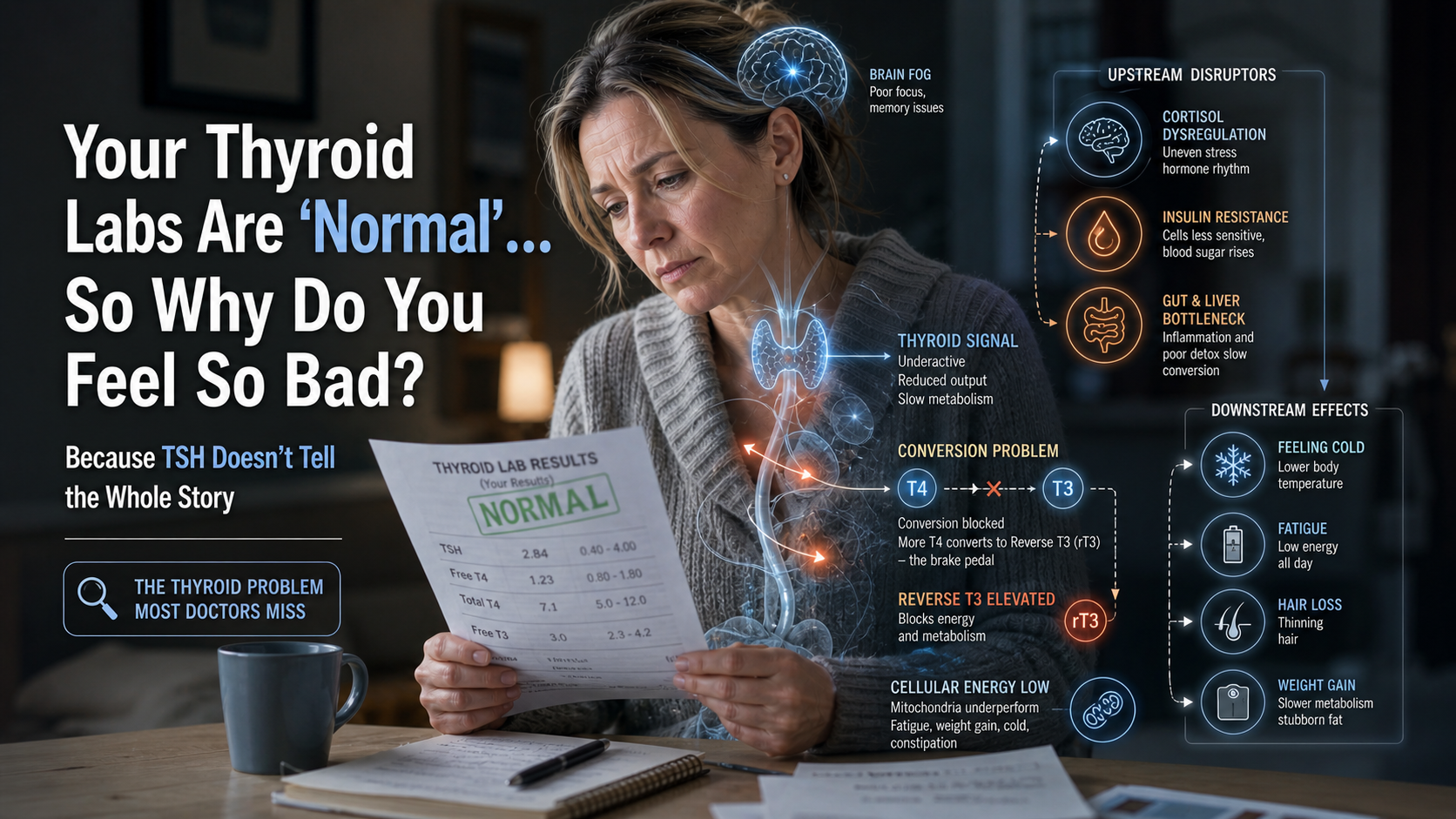
For decades I've watched the same scenario play out in my office. A woman in her 40s or 50s sits down, exhausted, cold, gaining weight, losing hair, and says, "My doctor says my thyroid is normal." She hands me labs showing a TSH of 2.8 or 3.5 and a "normal" free T4. She's been told there's nothing wrong.
There is something wrong. It's just not being measured correctly.
Subclinical thyroid dysfunction is one of the 14 core archetypes I see most frequently. It is rarely just a thyroid problem — it is almost always downstream of declining progesterone, rising insulin resistance, cortisol dysregulation, or gut inflammation.
Why Conventional Thyroid Testing Misses the Real Problem
Standard medicine relies heavily on TSH. When TSH is within the broad reference range (usually 0.4–4.0 or 0.5–5.0), the doctor stops looking. But TSH is a pituitary signal, not a direct measure of thyroid hormone activity at the cellular level.
What actually matters for how you feel:
- Free T3 (the active thyroid hormone)
- Reverse T3 (the brake pedal)
- Free T4 to Free T3 conversion efficiency
- Thyroid antibodies (TPO and TG) even if TSH is normal
Many patients have "normal" TSH but low-normal Free T3 and elevated Reverse T3 — the classic pattern of thyroid slowdown under stress or metabolic pressure.
The Real Cascade I See in Practice
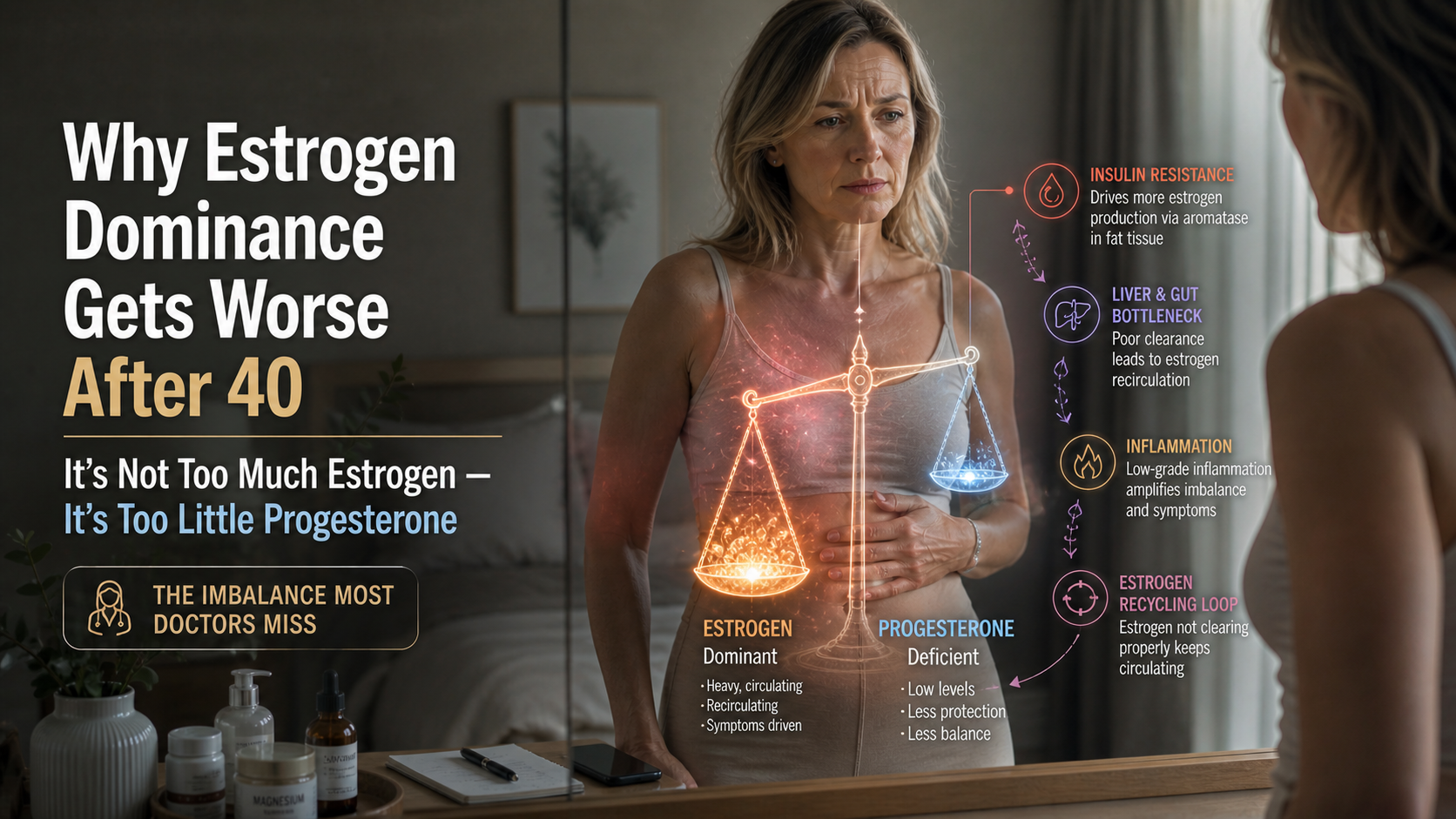
- Progesterone decline removes a major buffer against stress and insulin.
- Cortisol becomes dysregulated.
- Insulin resistance develops.
- Liver and gut function slow, impairing T4 to T3 conversion.
- The thyroid down-regulates to conserve energy — a protective response, not a disease.
This is why patients feel cold, constipated, mentally foggy, and metabolically stuck even when their doctor says everything is fine.
How I Approach Thyroid Dysfunction Clinically
I never start with thyroid medication alone. I start with the LCHPMF foundation because the thyroid is downstream of the other signals:
- Protein anchoring every meal to stabilize blood sugar and reduce insulin demand.
- Strategic carbohydrate timing to lower inflammation and support conversion.
- Cortisol rhythm restoration through consistent sleep and stress management.
- Gut and liver support — because poor clearance amplifies every thyroid problem.
Only after the foundation is solid do we look at targeted thyroid support if needed.
The free 3-minute assessment at Take the free Hormone & Metabolism Assessment will tell you if thyroid dysfunction is one of your active patterns. You'll receive a full Clinical Mirror report written in my voice and immediate access to LEO — my AI clinical assistant — who can walk you through the exact next steps.
If supplements are indicated, they are available at drjaywrigley.com with your automatic 15% patient discount.
Take the Assessment
It takes 3 minutes and may finally explain why you feel the way you do despite "normal" labs.
→ Start here: assessment.drjaywrigley.com
I read every reply. Tell me what pattern it shows for you. I'm here to help you get your energy and metabolism back.
— Dr. Jay Wrigley, NMD
Trusted Supplements
The supplements referenced in this article are available through Dr. Jay's practitioner dispensary.
Professional-grade formulations — the same brands used in clinical practice. 15% off retail, permanently. No membership required.
Browse Trusted Supplements →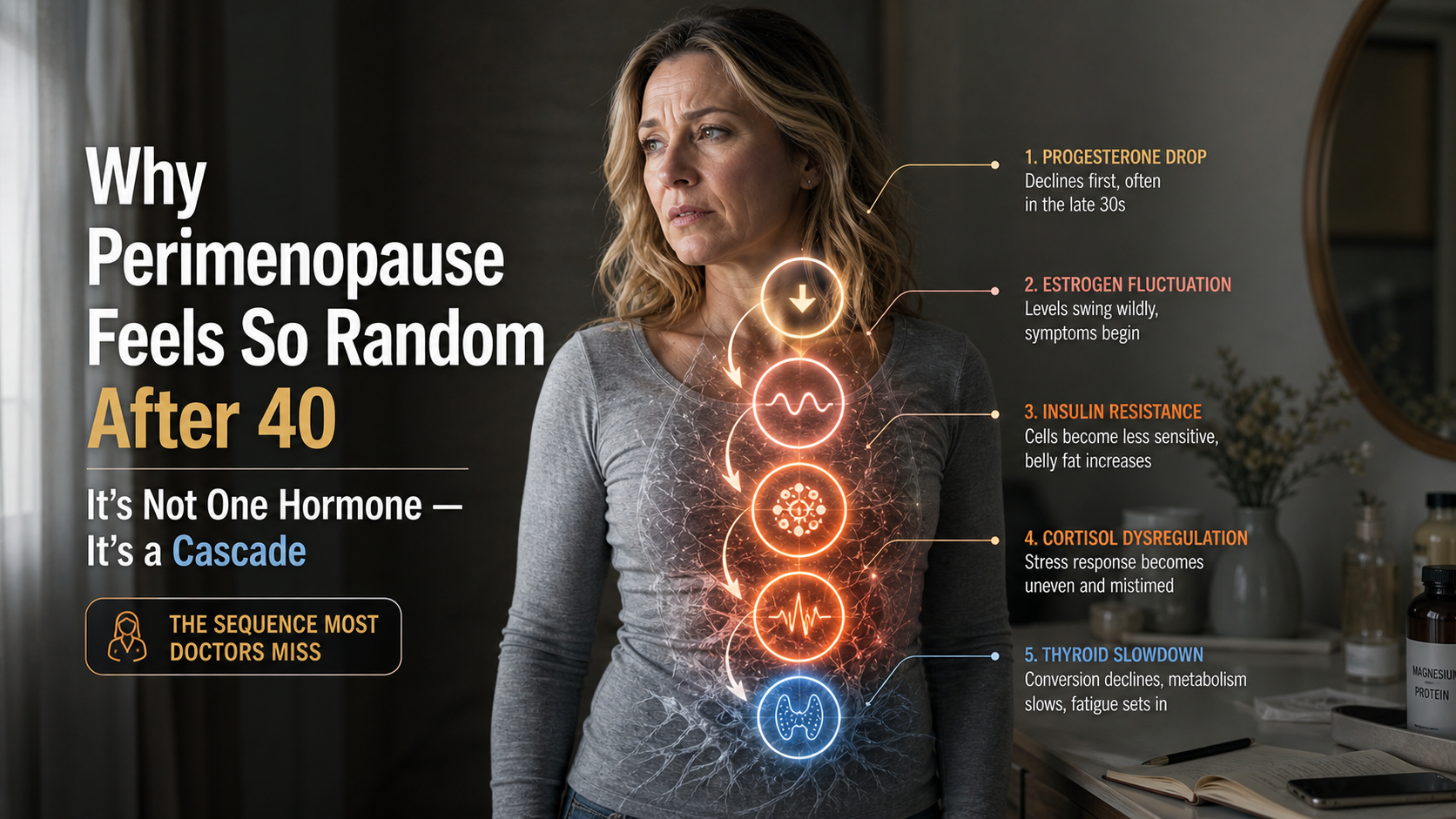
{kind=link}